
Health and Social Development Commission
Vision Statement
Through the full implementation of Treaties, First Nations powers, laws, and jurisdictions, we will develop a sound and responsive traditional, social, economic, and environmental infrastructure for the health benefit of our children and families and to deliver good quality services to all First Nations citizens, both on and off-reserve.
Commission Meetings
The Health and Social Development Commission (HSDC) is comprised of elected leadership appointed from the Tribal, Agency Grand Councils and the independent First Nations, and the FSIN Senate. The Executive Member with the Health and Social Development portfolio responsibility, Vice Chief Morley Watson, is the Chairperson of the Commission.
- Treaty Right to Health/Medicine Chest Task Force
- Health Governance
- Child Welfare Transformation - Ministry of Social Services
- Non Insured Health Benefits Program
- Policy Areas
- Suicide Prevention Strategy
- First Nations Addictions Rehabilitation Foundation
- SGI: Provincial Traffic Safety Fund Grant
Treaty Right to Health/Medicine Chest Task Force
First Nations possess constitutionally protected, Inherent and Treaty Rights to Health
The Inherent Rights to health and health care are granted by the Creator. First Nations are born with Inherent Rights and inherit them from generation to generation based on traditions, customs and practices. Inherent Rights include a traditional health system of: Medicine Women and Men; ceremonies and practices for healing and prevention; and medicines from minerals, animals, plants and water, traditional lands and resources. These are recognized and affirmed by the Constitution of Canada, common law, and international law.
Treaties are sacred covenants that were sanctified by prayers and ceremonies. First Nations law guided the leaders in their negotiations of the solemn agreements. The Treaties were carefully thought out by First Nation leaders with a lot of consideration given to securing a good life for future generations. Treaty 6 specifically includes the medicine chest clause as First Nations were fully aware of the new diseases and understood the importance of overall health. Treaty Commissioner Alexander Morris reports that the Indian people requested “provisions for the poor, unfortunate, blind and the lame” and “a free supply of medicines”.
The oral assurances and visual projections of medical aid and the provision of medical care during the Treaty negotiations were important to First Nations and form the basis for our understanding of the Treaty Right to Health. At the time Treaty was made, all Medicine chests contained the contemporary medicines of the period, as well as all the instruments used to compound, measure and dispense the drugs. Medical doctors often accompanied Treaty parties and dispensed medicine and provided medical care to demonstrate the health care available.
The Treaty Commissioner representing the Crown committed the following: “What you have will remain intact and what we have to offer you is on top of what you already have.” The First Nations had medicine bags (“mewut”) that contained medicine for the traditional health and health care system and the medicine chest is understood to provide for the contemporary health coverage and benefits.
It has been the long time position of First Nations that all health care and medicines are pre-paid and are to be provided to Treaty First Nations as promised in the Numbered Treaties. To this date, First Nations hold the Canadian government fully responsible for the cost of health care due to the legal obligations of Treaty. It is a Treaty Right that extends to all Numbered Treaties.
“The legal and political framework of the Inherent Rights and Powers, Treaties No. 1 to No. 11, the Royal Proclamation of 1763, the Constitution Act 1982, the International Laws and the United Nations Declaration on the rights of Indigenous Peoples recognizes the Inherent Rights and Treaty Rights to Health and Health Care for Indians.”-Senator Sol Sanderson
“For an understanding of the relationship between the Treaty Peoples and the Crown of Great Britain and later Canada, one must consider a number of factors beyond the treaty’s written text. First, the written text expresses only the government of Canada’s view of the treaty relationship: it does not embody the negotiated agreement. Even the written versions of treaties have been subject to considerable interpretation, and they may be scantily supported by reports or other information about the treaty negotiations.”-Sharon H. Venne, “Understanding Treaty 6: An Indigenous Perspective” in M. Asch, ed., Aboriginal and Treaty Rights in Canada (2002)
Health Governance
The overall goal is to implement the inherent and Treaty Right to Health by improving the quality of life for First Nations people through a culturally responsive health service delivery model. A First Nations Health Governance Strategy will target the planning and designing of a holistic health system that incorporates First Nations values, customs, and beliefs. All health related areas such as justice or education will be examined and encompassed in order to develop a health system that will improve the quality and access of health services for First Nations and First Nation communities. The FSIN continues to advocate to secure funding to complete the required phases of the governance plan.
A Special Assembly on Health took place on February 17 and 18, 2016 at Dakota Dunes Casino. The Assembly was a forum for First Nations leadership to discuss health governance and the issues that surround pertinent areas such as Treaty Right to Health. Discussion and direction from the floor called for a Strategy to be rolled up to include an administrative strategy, political strategy and legal strategy based on Inherent and Treaty Rights. This will include an education or awareness program on Treaty for the First Nations in the communities. As a means toward Treaty Implementation it was requested that a Jurisdictional and Sovereignty Implementation Action Plan be created. The importance of Treaty remained at the forefront of discussions. There was clear direction to be guided by the Treaty and not to compromise the Treaty or Inherent Rights to Health.
Child Welfare Transformation – Ministry of Social Services
Legislative Renewal: The Child and Family Services Act and the Adoption Act
The Ministry of Social Services is undertaking a review of the province’s child welfare legislation to ensure legislative and regulatory implications are fully considered for each of the Child Welfare Review Panel recommendations.
The Health and Social Development Commission is rejecting the proposed changes to the provincial legislation due to the lack of consultation.
National Policy Review:
In 1999, First Nations and INAC formed a joint National Policy ReviewCommittee to identify common concerns and develop recommendations to address the concerns. The Committee produced a report that identified significant funding issues resulting in a formula intended to provide equity, predictability and flexibility for ICFS Agencies. Despite the recommendations of this report, funding disparities continue. The Health and Social Development Commission recommends reinstating the National Policy Review Committee to review the Enhanced Funding Prevention Approach currently allocated by Canada.
National First Nations Commissioner on Child Welfare:
The Health and Social Development Commission recommended the development of a National First Nations Children’s Commissioner under the direction and control of First Nations. The role of this Commissioner is to address overrepresentation of First Nations children-in-care and to support children and families receiving services for the 133 First Nations CFS Agencies across Canada.
Non Insured Health Benefits Program
The NIHB program was established as Health Canada’s national, medically necessary health benefit program that provides coverage for benefit claims for a specified range of drugs, dental care, vision care, medical supplies and equipment, short-term crisis intervention mental health counselling and medical transportation for eligible First Nations people and Inuit.
Non-Insured Health Benefits Navigator
The FSIN staffs a Non-Insured Health Benefits Navigator to help support First Nations communities and individuals when refused or denied health benefits under their constitutionally protected rights. The FSIN continues to advocate on all received client calls requiring advocacy support.
AFN/FNIHB Joint Review
The Assembly of First Nations (AFN) and the First Nations and Inuit Health Branch (FNIHB) have undertaken a Joint Review of the Non-Insured Health Benefits (NIHB) Program with the following objectives:
- Enhance client access to benefits;
- Identify and address gaps in benefits;
- Streamline service delivery to be more responsive to client needs; and,
- Increase program efficiencies.
The NIHB Joint Review began in September 2014 after concerns were raised by First Nations, leading to advocacy efforts by First Nations leadership and the AFN. The review is guided by a Steering Committee made up of members from the Chiefs Committee on Health, the National First Nations Health Technicians Network and the National NIHB Navigators Network. The Steering Committee has equal representation from First Nations and FNIHB staff, including two Assistant Deputy Ministers with the authority to make program changes. The NIHB Joint Review is expected to be completed in 2017 and a final report with findings and recommendations will be presented.
Kāhui Tautoko Consulting Ltd (KTCL) has been contracted by the AFN to undertake this review. KTCL is a consultancy based in Vancouver, BC, specializing in First Nations health and communitydevelopment projects and has undertaken NIHB reviews previously. The objectives of this review are to determine:
- What processes are used to access these benefits and how effective these are;
- What challenges or barriers there are accessing these four benefits including awareness of what is available;
- If the NIHB program is meeting privacy and cultural needs; and
- The strengths and opportunities for improvement of the NIHB Program.
One of the current processes within the Joint Review is the operational benefits review which involves a series of community site visits that will consist of interviews with First Nation communities across the regions in Canada. The communities that have been selected by STAG based on criteria of geography, nature or level of contribution agreements, diversity of health services and needs, are the Onion Lake Cree Nation, Sturgeon Lake First Nation, Sakimay First Nation, Hatchet Lake First Nation, and Standing Buffalo First Nation.
National Non-Insured Health Benefits Working Group:
NIHB Navigators from several regions in Canada meet, along with AFN Technicians to present and discuss regional issues and challenges and work collaboratively to present recommendations to the Joint Review Process.
The last National NIHB meeting was held on October 21stand 22ndin Calgary, and the following issues were presented as an update:
- Jordan’s Principle
- Medical Transportation
- Accommodations for clients in urban areas
- Escorts are provided to clients
- Ambulance fees
- Drugs – the NIHB Drug List
- Dental care
- Vision Care
- Medical Supplies and Equipment
- Short Term Crisis Intervention Mental Health Counselling
NIHB Navigators will be presenting the following recommendations to the AFN Health Technician group, for their input into the Joint Review. It is important to note that further recommendations will be presented before the end of the Joint Review process, based on the community interviews that are being conducted by a contractor hired by the AFN. Health Technicians will be provided with information pertaining to the six communities that will be contacted in Saskatchewan and the process for identifying them based on criteria and specific parameters. Other discussions for recommendations were to have more Navigators hired in regions, and there were diverse opinions about the type of Navigators that each Region would require. For example, cancer care navigators, disability navigators, appeals navigators. Recommendations to AFN Health Technician Working Group:
- Dental centralization – propose that the centralization of dental and orthodontic pre-determination centre be moved back within the regions.
- Appeals – develop proposals to hire navigators to deal with appeals specifically.
- Cancer Care – develop proposal for cancer care Navigator to deal specifically with Cancer Care services in Saskatchewan.
- Meal Vouchers – proposal to develop loadable cards for NIHB Clients so they can have a choice for meals. This is similar to gift cards; instead, they will be for food purchases.
Policy Areas
Emergency Preparedness and Response
Memorandum of Understanding on Health and Wellness
The MOU Steering Committee (SC) was established to provide leadership in achieving the MOU goals to address closing the gaps in programs and services that First Nations continue to encounter. A key focus of the work of the MOU was to establish a process to develop a joint Saskatchewan First Nations Health and Wellness Plan (SFNHWP – hereinafter called “the Plan”). The draft Plan was completed as a high level strategic document and includes collaborative actions to improve health programs and services for First Nations in Saskatchewan.
Eight priority areas were identified and task groups were established with representatives from First Nations, Health Canada and the Saskatchewan Ministry of Health to develop specific options and recommendations for collaborative actions.
These include:
- Strengthening Health Human Resources
- Mental Health & Addictions
- Chronic Disease Prevention and Management
- Improving the Health Care System Experience
- Long Term Care
- Strengthening Relationships and Partnerships
- Intake & Discharge Planning
- E-Health
Cultural Responsiveness Framework
The Cultural Responsiveness Framework (CRF) is a foundational document that aims to foster improved relationships between First Nation individuals and communities and the health care institutions which serve them. Given the scope and significance of the CRF—which has the support of First Nations communities and addresses key recommendations in the Ministry of Health’s 2009 Patient First Review and the Truth and Reconciliation Commission (TRC) Calls to Action—CRF implementation has the potential to guide First Nations and mainstream health system engagement and collaboration towards a “middle ground” solution for meaningful, incremental, culturally responsive changes to the health care system. To achieve a more culturally responsive health care system, CRF implementation initiatives will require both community support and leadership support from mainstream health institutions—with an adequate, sustainable resource base for First Nations / health system engagement, research, key initiatives / demonstration projects, and evaluation. An evidence-based approach to measures systemic culturally responsive improvements also requires a sustainable resource base for data management and analysis capacity / infrastructure. Key partnership initiatives and demonstration projects—such as the Muskowekwan Residential School Education & Healing Centre initiative—will be used to: inform future evidence-based First Nations-led health policy revisions; establish a CRF Implementation Best Practices Guide; and support the further development of a CRF Performance Measurement Framework.
Elders, leadership, community members, both on and off-reserve, and others that hold a vested interest in the health of First Nations, have been consulted and their valuable insight and input are reflected into the draft CRF. Unions, educational institutions, RHA’s and other such stakeholders will be presented the CRF and given the opportunity to utilize the Framework document in building a safe, competent and responsive health care system in the province of Saskatchewan for First Nations members and communities.
The CRF and Literature Review were completed and passed by the Senior Technical Advisory Group and the Health and Social Development Commission Chiefs as part of the vetting process of FSIN.
First Nations Addictions & Rehabilitation Foundation (FNARF)
The Gaming Framework Agreement between the Federation of Saskatchewan Indian Nations and the Province of Saskatchewan provides for a review every five years during which time “Either Party may raise any matter for discussion and negotiation.” The 2002 Gaming Framework Agreement is a 25-year agreement with 5-year mandatory review periods.
The mandate of the First Nations Addiction Rehabilitation Foundation is to “work in cooperation with existing agencies and charities in order to ensure that effective and accessible prevention and treatment programs are available to First Nations people affected by gambling addictions.” The 2002 Gaming Framework Agreement between the FSIN and the Province of Saskatchewan states that the FSIN “established FNARF to ensure that effective and accessible education, prevention, and treatment programs about problem gambling are available to First Nations people.”
First Nations Regional Health Survey (RHS)
The First Nations Information Governance Centre (FNIGC), a premier research and data centre in Ottawa, works with 10 regions throughout Canada to collect credible, reliable data on the traditional and western health well-being of on-reserve First Nations. In Saskatchewan, FSIN works in collaboration with FNIGC to oversee the RHS project. FSIN previously implemented a sample plan that mirrors the geo-political regions/Tribal Councils recognized by the FSIN to ensure that all communities have an opportunity to participate. 70 First Nations in 10 Tribal Council and multi-communities and 10 independent First Nations have been invited to participate in the RHS phase 3 project. FSIN RHS staff are responsible to engage all First Nation communities to participate in the RHS project, support sub-regional manager and fieldworker staff training and monitor data collection for quality control. RHS staff is will ensure accountability to the First Nation communities by providing a sub-regional level report on the results upon completion of data collection. The FSIN Health and Social Development Secretariat will support Tribal Councils and communities to meet their target sample for maximum reliability of their data. The project completion date is September 30, 2016 with a target of 5,455 in the 70 First Nations.
Telehealth / e-Health
In 2004, the Government of Canada granted Canada Health Infoway (CHI) the mandate to work with Canada’s provincial/territorial governments to develop a public health surveillance system for all jurisdictions. The product that was delivered by this project is called Panorama. The province of Saskatchewan is currently implementing Panorama as its public health surveillance system. Panorama is a web-based software application that will be used as a replacement for the Saskatchewan Immunization Management System (SIMS).
There is a two-project team approach to deploying Panorama in Saskatchewan. The Government of Saskatchewan is currently deploying Panorama in stages as it determines the readiness of each Panorama module. The First Nations Deployment of Panorama in Saskatchewan (FNDPS) project is a separate project that follows the Provincial implementation of Panorama. The goal of the FNDPS project is to support planning and alignment activities with the Provincial project to ensure Panorama can be of benefit to the First Nation communities in Saskatchewan; and that communities have the information to make an informed choice before subscribing to Panorama.
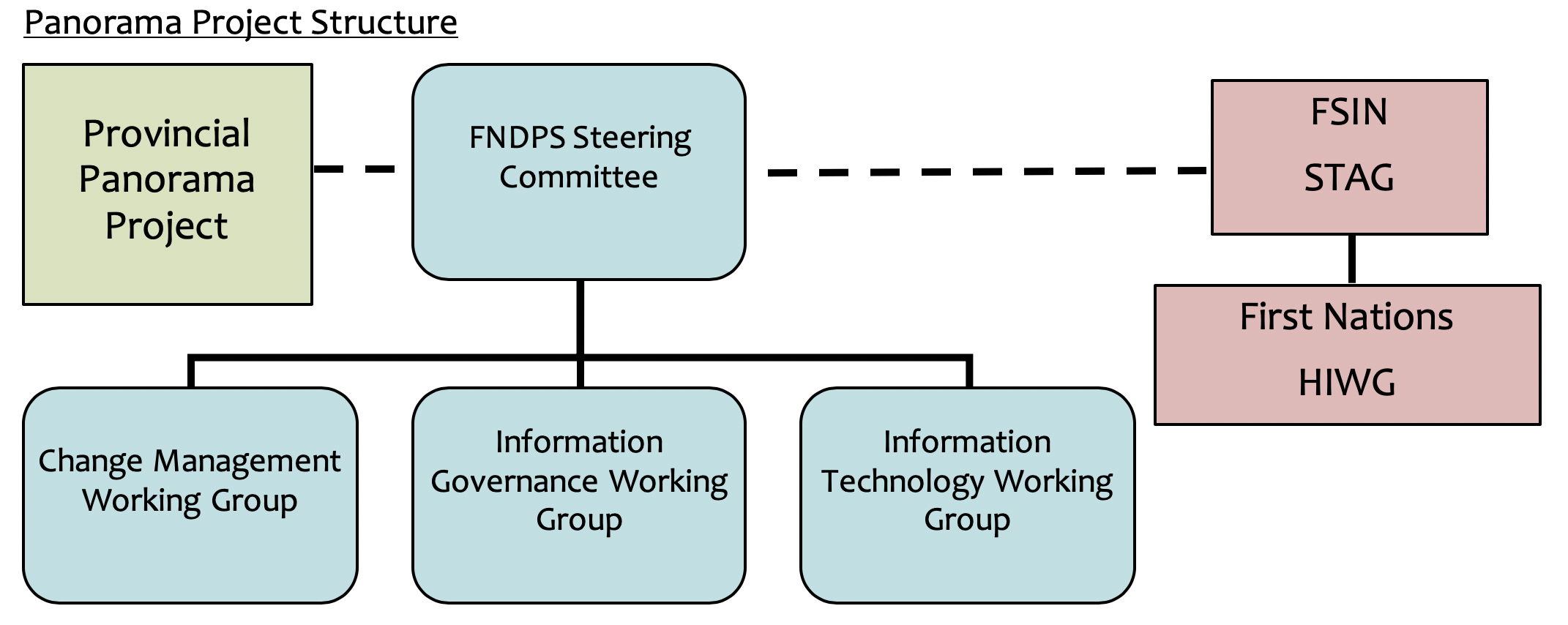
Panorama Project Structure
The Province of Saskatchewan deployed the Inventory module of Panorama in March of 2014. The inventory module was made available to all First Nation immunization depot sites including Northern Inter-Tribal Health Authority; South Service Centre; North Service Centre; Spiritwood; Saskatoon Tribal Council; Onion Lake; and Battle River Treaty 6. The deployment of the Immunization module was implemented in February 2015.
The Saskatchewan Provincial Panorama Project implemented the Inventory and Immunization modules of Panaroma along with First Nation communities that were previously using SIMS. First Nation communities that are not using SIMS but that are ready to implement Panorama have faced information governance issues. The provincial government has continued to use the SIMS information governance model for their deployment of Panorama.
With the current Inventory and Immunization modules now deployed the FNDPS project is discontinuing the Change Management and Information Technology working groups. The Steering committee will continue, to evaluate the governance options from the provincial government and all other Panorama business. The Information Governance working group will continue in a loose capacity but only meet when assigned work by the steering committee.
Environmental Health / Drinking Water Safety
Safe Drinking Water Baseline Study:
In 2006 and 2010 FSIN facilitated a Water Sampling project on all 74 First Nations in Saskatchewan. The objective is to:
- Document the present water quality of the communal drinking water systems;
- Determine the potential health effects and local concerns with the water supply infrastructure;
- Disseminate these results to the respective community in accordance with the Principles of OCAP and
- Increase capacity in the areas of the water quality support and testing systems.
AFN First Nations Food Nutrition Environment Study
David Suzuki Foundation MOU
Water Regulations Development and Water Conference:
FSIN held a Water Forum March 9-10 at the Saskatoon Travelodge. The forum was an opportunity to provide information on the Saskatchewan First Nations on the Safe Drinking Water Act review, solicit feedback and recommendations on the review, and hear from technicians and experts on various water and environmental initiatives across Canada. Based on comments from First Nations technicians at the forum, FSIN will create a report to lead discussions on the development of regulations, including the option of using the experience of technicians and past initiatives to look at a “source to tap” regulatory agency.
Saskatchewan First Nations Technical Services Co-operative (SFNTSC):
On May 28, 2015 the Chiefs of the Legislative Assembly passed Resolution 1964 to approve the establishment of a Tribal/Agency/Grand Council Technical Services Co-operative. The SFNTSC was incorporated on October 15, 2015.
The Co-operative is wholly owned by First Nations who choose to become members and governed by a Board composed of one representative from each Saskatchewan Tribal/Agency/Grand Council and one from among the Independent First Nations. The SFNTSC is not an entity or institution of FSIN. The role of the Co-operative is to support Tribal/Agency/Grand Councils by ensuring they continue as technical service providers to First Nations and by developing and offering services in areas currently outsourced by Tribal/Agency/Grand Councils to non-First Nations companies and organizations, including those provided by provincial and federal governments.
Office of Disabilities
The office of Disabilities works with First Nations Person(s) and their families in navigating the health services available to them, working to ensure:
- Adequacy – People with disabilities should have an adequate income that truly meets their needs without the indignity of having to justify their needs.
- Hope & Security – People with disabilities must have financial accommodations so that they can live their lives with hope, respect and dignity instead of a system of disincentives.
- Person-Centered and User Friendly – People with disabilities should be able to expect a dignified service that focuses on their individual financial needs as its reason for being.
- Higher Income Exemptions – People with disabilities need to be adequately accommodated as they move into training or employment.
An Annual Disability Golf Fundraiser raises funds for future initiatives and events for First Nations with Disabilities. The Sask First Nation Four Person Scramble Disability Golf Tournament will be held on September 22, 2016 at the Dakota Dunes Golf Links in Whitecap, Saskatchewan.
Letter of Understanding between the FSIN and Advocate for Children and Youth
FSIN and Saskatchewan Advocate for Children and Youth signed a Letter of Understanding on September 18, 2012. The Saskatchewan Advocate for Children and Youth (ACY) is an independent office of the Legislative Assembly of Saskatchewan. The mandate of the office is to advocate and investigate matters affecting children who are receiving or have been denied a service from Saskatchewan.
Through our Letter of Understanding, both the FSIN and the Advocate are solidifying our shared aspirations, interests and goals to keep children safe, to foster a system that nurtures children and families, that breaks down the stigma associated with asking for help, and to promote the rights and entitlements of First Nations children and youth, on and off-reserve.
Aboriginal Head Start On-Reserve Program and Childcare Initiatives
The Aboriginal Headstart On-Reserve Program delivers programs to 79 sites in the 74 communities in Saskatchewan, The FSIN Health and Social Development Secretariat (HSDS) Aboriginal Headstart Program manager is responsible for coordinating and monitoring for the 10 Independent First Nations to support them, in meeting their program objectives and deliverables. The AHS program manager role is also to advocate for the 74 First Nations of Saskatchewan, at both Regional and National levels.
Saskatchewan First Nations have been participating in the First Nations and Inuit Child Care Initiatives since 1995. There are currently 74 on-reserve centers throughout Saskatchewan. The FSIN Health & Social Secretariat Early Learning & Child Care program is responsible to support the regional and national delivery of the First Nations/Inuit Child Care programs in Saskatchewan. The Early Learning & Child Care program continues to be committed to the licensing and monitoring of Independent First Nations childcare programs and ensuring quality programming for Independent First Nations Daycare Centers.
The program manager for both Head Start and Daycare coordinates and organizes regular FNECC working group meetings, to support the work and strategies of the First Nations Early Childhood Circle. The First Nations Early Childhood Circle (FNECC) was established to provide leadership, input, technical support and guidance to the Saskatchewan Technical Advisory Group (STAG) and then to the Commissions on all issues related to early childhood development and other related children’s issues.
Saskatchewan First Nations/Inuit Child Care Initiatives Agreements are on the last stage of their Agreements with the 74 First Nations across Saskatchewan, the Agreement came to an end March 31, 2015. New Agreements for the Child Care Initiative have currently been extended to March 2017, and are currently being discussedat the NationalLevel with no word to day as to the amount of funding for Saskatchewan Region and each of the 74 First Nation Communities. A Planning committee has been established to develop a new Childcare Strategy for the Child Care Programs Nationally, with a goal to meet and develop and strategize possible ways to increase funding to all of the 74 First Nations Daycares in Saskatchewan.
The FNECC working group has developing Training for front line Early Learning and Child Care providers to use the Saskatchewan First Nations Early Learning and Child Care Policy and Regulations in their Early Learning and Childcare sites. The working group revised and updated the Policy and Regulations so that they are equal to or exceed the Provinces and Tribal Councils Policy and Regulations. The Policy and regulations are intended to guide Early Childhood Programming in Saskatchewan First Nations Aboriginal Head start and Daycare Centers and to enhance safety and quality programming in all early learning programs.
The FNECC working group has developed a workshop for First Nations Leadership, Principals, Director of Health and Education, Portfolio holders, and those that work within the First Nations Early Learning and Childcare Program in First Nations Communities. This workshop will be to educate all those involved in Children’s programs, and provide information what the Aboriginal Headstart and Daycare Programs entail. This workshop will be delivered annually or when needed to First Nations communities across Saskatchewan.
With the Renewal of all the Childcare Program Nationally in March 2017, the FNECC committee have been conducting an Early Learning and Childcare Environmental Assessment Scan that is evaluating all the early learning and childcare programs across the 74 First Nations in Saskatchewan. This Assessment will evaluate the needs for better outcomes in addressing the gaps in services and resources of early learning programs in Saskatchewan and by increasing the funding formula to include current population stats of communities and the cost of living Index of today.
The FNECC working group hosted a Successful Early Learning and Childcare Summit in February 2016 that brought Front line First Nations Aboriginal Head Start on Reserve and Childcare providers to Saskatoon for a 3-day summit that included workshops in all area of children’s programs.
Areas the FNECC working group will be working on in 2016-2017 fiscal year are:
- Training on Policy and Regulations for Early Learning Programs
- Early Learning and Childcare Framework
- Early Learing and Childcare Website
- Special Needs
- Assessment and Evaluation of Childcare Programs
- On-going Workshop for Leadership, Principals, Portfolio holders, to enhance and promote Early Learning and Childcare programs.
- Strategic Plan for Daycare Seats/Allocations
- Aboriginal Headstart 6 Components
- Training on Monitoring Procedures to Early Learning and Childcare Centres
- Curriculum Development for Early Learning Programs
Coalitions Linking Action and Science for Prevention(CLASP)
Coalitions Linking Action and Science for Prevention (CLASP) is an initiative of the Canadian Partnership Against Cancer (CPAC). The goal of CLASP is for organizations from various provinces and territories to form coalitions with the purpose of reducing risk factors for cancer and chronic diseases. CPAC funded seven (7) projects; one of which had FSIN as the lead agency.
The FSIN-led project was called Health Empowerment for You (HEY). The three project outcomes are: partnership development; curriculum development; and creating sustainable actions. The first two outcomes have been completed; partners are working towards securing sustainable project resources.
Partnership development included working with 14 partner agencies in the provinces of Manitoba and Saskatchewan. Partnering with FSIN are Manitoba First Nations, Health Canada, Manitoba Health, Saskatchewan Health, post-secondary institutions, and cancer and chronic disease agencies. For many project partners this is the first time that they have collaborated to improve First Nations health.
The HEY curriculum promotes healthy living to youth as a way to reduce risk factors for cancer and chronic disease in Manitoba and Saskatchewan First Nations. There were many conversations with Elders, youth and communities to ensure that the content is relevant for use at the community level. Holistic health is an important component of the HEY curriculum. The curriculum content is respectful of First Nations and has created linkages between non-First Nations health care with First Nations health traditions. The HEY curriculum consists of seven (7) modules: Vision of Health; Prevention of Cancer and Chronic Disease; Healthy Eating; Active Living; Healthy Body for Me; Smoke Free; and Avoid Misuse of Substances. Each module is to raise awareness of common risk factors for cancer and chronic disease, and promote change to healthy living. Participants learn how to plan a change in their behaviors; including planning to overcome challenges along as they implement the plan. Health Empowerment for You has completed its original mandate, but the project partners continue to collaborate. The next goal is to achieve project sustainability which includes the continued deployment and evaluation of the HEY curriculum.
The CLASP project has trained 105 people to facilitate the healthy living message to youth, including 68 from Saskatchewan. Trainers have been using the HEY holistic health messaging in their communities. Evaluation of curriculum has been rated as excellent Best Practice First Nation model and Public Health Agency will review a plan to post on its newly developing First Nation Best Practice models for First Nation members and communities.
Several requests from across Canada have been received for HEY curriculum and training and are on hold until sustainable capacity and resources are accessed. Discussions and meetings are ongoing to explore partnership with Manitoba First Nation Education Resource Council to explore adaption of curriculum to classroom use in all First Nation schools in Manitoba. Health Empowerment for You (HEY) still meets on quarterly basis and are in process of planning next steps and researching resource acquisition for further implementation of HEY in Saskatchewan.
Cancer Surveillance & Monitoring Project: Funding for project was accessed for 2014-2017 through the First Nation, Inuit & Metis Cancer Control Initiative. Lead partner on this Project is Saskatchewan Cancer Agency as FSIN did not have the professional capacity of epidemiologist to assist in data collection and surveillance. Co-partner is Metis Nation-Saskatchewan. This partnership is a first in Canada where three partners were approved funding to enable development of patient identification system for First Nations & Metis people. Saskatchewan Cancer Agency has no system in place to track First Nation clients who enter the cancer care system. We have three First Nation partners Ochapowace, English River and Battle River Treaty 6 Health Clinic participating in Project. Once tracking system is in place we will have cancer statistics in the communities that will enable us to identify number of clients, types of cancer and treatment within the system and in community. At end of project we should have a continuum of care developed for cancer care for First Nation clients. Including discharge planning, navigation, cultural responsive resources and services, access to care in remote and rural communities and community based health human resource skills and capacity and community awareness. Research is now completed with First Nation cancer clients and caregivers.
A partnership was formed in early March and proposal was submitted for Nourishing Garden Project another 3 project where three pilot schools Cote, Keeseekoose and Ochapowace were funded to plant a garden at the school in order for students to consume more vegetables. To date gardens have been planted and on-going meetings for planning and preparing harvest of vegetables with students, parents, elders and teachers are occurring at community level. Part of this project is evaluation and development of healthy school public policy in areas of nutrition, exercise guided by cultural history and teachings and values. Year 2 of Project will focus on evaluation of Project, teachers, students and will be completed by Propel from Waterloo, University of Ontario.
The Province of Saskatchewan deployed the Inventory module of Panorama in March of 2014. The inventory module was made available to all First Nation immunization depot sites including Northern Inter-Tribal Health Authority; South Service Centre; North Service Centre; Spiritwood; Saskatoon Tribal Council; Onion Lake; and Battle River Treaty 6. The deployment of the Immunization module was implemented in February 2015.
The Saskatchewan Provincial Panorama Project implemented the Inventory and Immunization modules of Panaroma along with First Nation communities that were previously using SIMS. First Nation communities that are not using SIMS but that are ready to implement Panorama have faced information governance issues. The provincial government has continued to use the SIMS information governance model for their deployment of Panorama. The SIMS model does not currently allow for new organizations to be easily added to their existing agreements. The province is evaluating legal options for deploying Panorama to non-SIMS First Nations communities.
With the current Inventory and Immunization modules now deployed the FNDPS project is discontinuing the Change Management and Information Technology working groups. The Steering committee will continue, to evaluate the governance options from the provincial government and all other Panorama business. The Information Governance working group will continue in a loose capacity but only meet when assigned work by the steering committee.
The FSIN continues to revise and vet our legal review document of information governance and data exchange through First Nation governments. Revisions and vetting of the First Nations eHealth strategy document also continues. In the New Year, work on the Panorama project will continue to address the information governance options for using the Panorama software.
Environmental Health / Drinking Water Safety
Safe Drinking Water Baseline Study:
In 2006 and 2010 FSIN facilitated a Water Sampling project on all 74 First Nations in Saskatchewan. The objective is to:
- Document the present water quality of the communal drinking water systems;
- Determine the potential health effects and local concerns with the water supply infrastructure;
- Disseminate these results as widely as possible in order to educate the people involved in the delivery and monitoring of these water supply systems and to effect changes in procedures, approach and regulations; and
- Increase capacity in the areas of the water quality support and testing systems.
AFN First Nations Food Nutrition Environment Study
David Suzuki Foundation MOU
Water Regulations Development and Water Conference:
FSIN held a Water Forum for March 9-10 at the Saskatoon Travelodge. The forum was an opportunity to provide information to Saskatchewan First Nations on the Safe Drinking Water Act review, solicit feedback and recommendations on the review, and hear from technicians and experts on various water and environmental initiatives across Canada. Based on comments from First Nations technicians at the forum, FSIN will create a report to lead discussions on the development of regulations, including the option of using the experience of technicians and past initiatives to look at a “source to tap” regulatory agency.
Saskatchewan First Nations Technical Services Co-operative (SFNTSC)
On May 28, 2015 the Chiefs of the Legislative Assembly passed Resolution 1964 to approve the establishment of a Tribal/Agency/Grand Council Technical Services Co-operative. The SFNTSC was incorporated on October 15, 2015.
The Co-operative is wholly owned by First Nations who choose to become members and governed by a Board composed of one representative from each Saskatchewan Tribal/Agency/Grand Council and one from among the Independent First Nations. The SFNTSC is not an entity or institution of FSIN. The role of the Co-operative is to support Tribal/Agency/Grand Councils by ensuring they continue as technical service providers to First Nations and by developing and offering services in areas currently outsourced by Tribal/Agency/Grand Councils to non-First Nations companies and organizations, including those provided by provincial and federal governments.
Office of Disabilities
The office of Disabilities works with First Nations Person(s) and their families in navigating the health services available to them, working to ensure:
- Adequacy – People with disabilities should have an adequate income that truly meets their needs without the indignity of having to justify their needs.
- Hope & Security – People with disabilities must have financial accommodations so that they can live their lives with hope, respect and dignity instead of a system of disincentives.
- Person-Centered and User Friendly – People with disabilities should be able to expect a dignified service that focuses on their individual financial needs as its reason for being.
- Higher Income Exemptions – People with disabilities need to be adequately accommodated as they move into training or employment.
An Annual Disability Golf Fundraiser raises funds for future initiatives and events for First Nations with Disabilities. The Sask First Nation Four Person Scramble Disability Golf Tournament was held on Thursday June 9th2016 at the Dakota Dunes Golf Links in Whitecap, Saskatchewan.
Letter of Understanding between the FSIN and Advocate for Children and Youth
FSIN and Saskatchewan Advocate for Children and Youth signed a Letter of Understanding on September 18, 2012. The Saskatchewan Advocate for Children and Youth (ACY) is an independent office of the Legislative Assembly of Saskatchewan. The mandate of the office is to advocate and investigate matters affecting children who are receiving or have been denied a service from Saskatchewan.
Through our Letter of Understanding, both the FSIN and the Advocate are solidifying our shared aspirations, interests and goals to keep children safe, to foster a system that nurtures children and families, that breaks down the stigma associated with asking for help, and to promote the rights and entitlements of First Nations children and youth, on and off-reserve.
Aboriginal Head Start On-Reserve Program and Childcare Initiatives
The Aboriginal Headstart On-Reserve Program delivers programs to 79 sites in the 74 communities in Saskatchewan, The FSIN Health and Social Development Secretariat (HSDS) Aboriginal Headstart Program manager is responsible for coordinating and monitoring for the 10 Independent First Nations to support them, in meeting their program objectives and deliverables. The AHS program manager role is also to advocate for the 74 First Nations of Saskatchewan, at both Regional and National levels.
Saskatchewan First Nations have been participating in the First Nations and Inuit Child Care Initiatives since 1995. There are currently 74 on-reserve centers throughout Saskatchewan. The FSIN Health & Social Secretariat Early Learning & Child Care program is responsible to support the regional and national delivery of the First Nations/Inuit Child Care programs in Saskatchewan. The Early Learning & Child Care program continues to be committed to the licensing and monitoring of Independent First Nations childcare programs and ensuring quality programming for Independent First Nations Daycare Centers.
The program manager for both Head Start and Daycare coordinates and organizes regular FNECC working group meetings, to support the work and strategies of the First Nations Early Childhood Circle. The First Nations Early Childhood Circle (FNECC) was established to provide leadership, input, technical support and guidance to the Saskatchewan Technical Advisory Group (STAG) and then to the Commissions on all issues related to early childhood development and other related children’s issues.
Saskatchewan First Nations/Inuit Child Care Initiatives Agreements are on the last stage of their Agreements with the 74 First Nations across Saskatchewan, the Agreement came to an end March 31, 2015. New Agreements for the Child Care Initiative have currently been extended to March 2017, and are currently being discussed at the National Level with no word to day as to the amount of funding for Saskatchewan Region and each of the 74 First Nation Communities. A Planning committee has been established to develop a new Childcare Strategy for the Child Care Programs Nationally, with a goal to meet and develop and strategize possible ways to increase funding to all of the 74 First Nations Daycares in Saskatchewan.
The FNECC working group has developing Training for front line Early Learning and Child Care providers to use the Saskatchewan First Nations Early Learning and Child Care Policy and Regulations in their Early Learning and Childcare sites. The working group revised and updated the Policy and Regulations so that they are equal to or exceed the Provinces and Tribal Councils Policy and Regulations. The Policy and regulations are intended to guide Early Childhood Programming in Saskatchewan First Nations Aboriginal Head start and Daycare Centers and to enhance safety and quality programming in all early learning programs.
The FNECC working group has developed a workshop for First Nations Leadership, Principals, Director of Health and Education, Portfolio holders, and those that work within the First Nations Early Learning and Childcare Program in First Nations Communities. This workshop will be to educate all those involved in Children’s programs, and provide information what the Aboriginal Headstart and Daycare Programs entail. This workshop will be delivered annually or when needed to First Nations communities across Saskatchewan.
With the Renewal of all the Childcare Program Nationally in March 2017, the FNECC committee have been conducting an Early Learning and Childcare Environmental Assessment Scan that is evaluating all the early learning and childcare programs across the 74 First Nations in Saskatchewan. This Assessment will evaluate the needs for better outcomes in addressing the gaps in services and resources of early learning programs in Saskatchewan and by increasing the funding formula to include current population stats of communities and the cost of living Index of today.
The FNECC working group hosted a Successful Early Learning and Childcare Summit in February 2016 that brought Front line First Nations Aboriginal Head Start on Reserve and Childcare providers to Saskatoon for a 3-day summit that included workshops in all area of children’s programs.
Areas the FNECC working group will be working on in 2016-2017 fiscal year are:
- Training on Policy and Regulations for Early Learning Programs
- Early Learning and Childcare Framework
- Early Learing and Childcare Website
- Special Needs
- Assessment and Evaluation of Childcare Programs
- On-going Workshop for Leadership, Principals, Portfolio holders, to enhance and promote Early Learning and Childcare programs.
- Strategic Plan for Daycare Seats/Allocations
- Aboriginal Headstart 6 Components
- Training on Monitoring Procedures to Early Learning and Childcare Centres
- Curriculum Development for Early Learning Programs
Coalitions Linking Action and Science for Prevention (CLASP)
Coalitions Linking Action and Science for Prevention (CLASP) is an initiative of the Canadian Partnership Against Cancer (CPAC). The goal of CLASP is for organizations from various provinces and territories to form coalitions with the purpose of reducing risk factors for cancer and chronic diseases. CPAC funded seven (7) projects; one of which had FSIN as the lead agency.
The FSIN-led project was called Health Empowerment for You (HEY). The three project outcomes are: partnership development; curriculum development; and creating sustainable actions. The first two outcomes have been completed; partners are working towards securing sustainable project resources.
Partnership development included working with 14 partner agencies in the provinces of Manitoba and Saskatchewan. Partnering with FSIN are Manitoba First Nations, Health Canada, Manitoba Health, Saskatchewan Health, post-secondary institutions, and cancer and chronic disease agencies. For many project partners this is the first time that they have collaborated to improve First Nations health.
The HEY curriculum promotes healthy living to youth as a way to reduce risk factors for cancer and chronic disease in Manitoba and Saskatchewan First Nations. There were many conversations with Elders, youth and communities to ensure that the content is relevant for use at the community level. Holistic health is an important component of the HEY curriculum. The curriculum content is respectful of First Nations and has created linkages between non-First Nations health care with First Nations health traditions. The HEY curriculum consists of seven (7) modules: Vision of Health; Prevention of Cancer and Chronic Disease; Healthy Eating; Active Living; Healthy Body for Me; Smoke Free; and Avoid Misuse of Substances. Each module is to raise awareness of common risk factors for cancer and chronic disease, and promote change to healthy living. Participants learn how to plan a change in their behaviors; including planning to overcome challenges along as they implement the plan. Health Empowerment for You has completed its original mandate, but the project partners continue to collaborate. The next goal is to achieve project sustainability which includes the continued deployment and evaluation of the HEY curriculum.
The CLASP project has trained 105 people to facilitate the healthy living message to youth, including 68 from Saskatchewan. Trainers have been using the HEY holistic health messaging in their communities. Evaluation of curriculum has been rated as excellent Best Practice First Nation model and Public Health Agency will review a plan to post on its newly developing First Nation Best Practice models for First Nation members and communities.
Several requests from across Canada have been received for HEY curriculum and training and are on hold until sustainable capacity and resources are accessed. Discussions and meetings are ongoing to explore partnership with Manitoba First Nation Education Resource Council to explore adaption of curriculum to classroom use in all First Nation schools in Manitoba. Health Empowerment for You (HEY) still meets on quarterly basis and are in process of planning next steps and researching resource acquisition for further implementation of HEY in Saskatchewan.
Cancer Surveillance & Monitoring Project: Funding for project was accessed for 2014-2017 through the First Nation, Inuit & Metis Cancer Control Initiative. Lead partner on this Project is Saskatchewan Cancer Agency as FSIN did not have the professional capacity of epidemiologist to assist in data collection and surveillance. Co-partner is Metis Nation-Saskatchewan. This partnership is a first in Canada where three partners were approved funding to enable development of patient identification system for First Nations & Metis people. Saskatchewan Cancer Agency has no system in place to track First Nation clients who enter the cancer care system. We have three First Nation partners Ochapowace, English River and Battle River Treaty 6 Health Clinic participating in Project. Once tracking system is in place we will have cancer statistics in the communities that will enable us to identify number of clients, types of cancer and treatment within the system and in community. At end of project we should have a continuum of care developed for cancer care for First Nation clients. Including discharge planning, navigation, cultural responsive resources and services, access to care in remote and rural communities and community based health human resource skills and capacity and community awareness. Research is now completed with First Nation cancer clients and caregivers.
A partnership was formed in early March and proposal was submitted for Nourishing Garden Project another 3 project where three pilot schools Cote, Keeseekoose and Ochapowace were funded to plant a garden at the school in order for students to consume more vegetables. To date gardens have been planted and on-going meetings for planning and preparing harvest of vegetables with students, parents, elders and teachers are occurring at community level. Part of this project is evaluation and development of healthy school public policy in areas of nutrition, exercise guided by cultural history and teachings and values. Year 2 of Project will focus on evaluation of Project, teachers, students and will be completed by Propel from Waterloo, University of Ontario.
Suicide Prevention Strategy
Download SPS Community Engagement Letter
Download SK FN SPS Discussion Paper
First Nations Addictions Rehabilitation Foundation
Mission Statement
The First Nation Addiction Rehabilitation Foundation is dedicated to helping First Nations people in Saskatchewan by promoting responsible gambling. The mission of FNARF is to promote and maintain healthy lifestyles that enhance healthy individuals, families and communities by increasing the use of holistic approaches. It accomplishes this mission by engaging in activities in four mandated areas: education, prevention, research and treatment.
What does FNARF do?
FNARF is a program made available at the tribal council or independent grassroots level. Funding is provided by the Saskatchewan Indian Gaming Authority to ensure education, prevention and treatment programs and services are available to First Nations people dealing with gambling addictions. In 2007 research into problem gambling was added to the FNARF mandate.
What is Responsible Gambling?
For many First Nations and Aboriginal people, gambling is considered a social activity. Playing bingo, dropping a couple of bucks into a machine, wagering on horse racing, or just going over to the local store and buying a lottery ticket.
Responsible gaming occurs when informed participants have a clear understanding of the probabilities of winning and engage in low risk gaming situations and wager reasonalble amounts.
“Knowing your limit and playing within it”
(reprint in part from Saskatchewan Responsible Gaming Association)
What is Problem Gambling Behaviour?
Problem gambling behaviour can affect significant areas of a person’s life. This may include health, employment, financial, and famliy relationships.
High-risk problem gambers usually are borrowing this money with every intention of repaying it. But realistically that individual is having noticeable negative effects in areas of their life, such s excessive debt, marital problems or illegal activity.
Theories of Problem Gambling
The FNARF Board of Driectors realizes that there are many theories, models and approaches to assist those experiencing gambling related difficulties.
Currently, the FNARF Board of Directors recognizes three models in dealing with Problem Gambling. The “Controlled/Risk Reduction Model,” the “Disease/Abstinence Model” and the “Circle of Care” model.
With the “Controlled/Risk Reduction Model” one maintains that people can be social gamblers and can gamble for recreation and not have a problem with gambling.
The “Disease/Abstinence Model” recognizes there will be persons who will develop major gambling problems and the only recourse is abstinence.
The “Circle of Care” model encompasses the medicine wheel teachings and holistic approaches to healthy living.
Preventing Problem Gambling
For many people gambling is exciting and entertaining. They make careful decisions about spending time and money, where to go and how to have fun. Here’s how to avoid problems:
Gambling for entertainment, not as a way to make money. The house always has the advantage. You are really just paying to play the game. Make sure you know how the game works and what the odds are before you decide to play. Only use discretionary income, not money for everyday expenses. Set a budget and stick to it. Do not use cash machines to get more money for gambling. Leave your debit and credit card at home when you decide to gamble. Set a time limit. Take frequent breaks. Be aware-risk increases at time of loss or depression. Don’t borrow money to gamble. Do not ‘chase’ losses. Accept them as the cost of entertainment. Balance gambling with other leisure activities.
(reprinted in part from the Responsible Gambing Council of Ontario)
Harm-Minimization Strategy
The Board of Directors of the First Nations Addictions Rehabilitation Foundation has developed a Regional Strategy on Problem Gambling behaviours. Many of the First Nations communities in Saskatchewan are currently implementing “Harm-Reduction Strategies” within their health and social community programming for problem gambling. Support must continue for the Problem Gambling Services to minimize gaps in services for those seeking help with problem gambling.
The FNARF Board of Directors maintaing a position to neither endorse nor opposes the gaming industry. Thus, in developing the regional strategy, respect and recognition is granted to legalized gambling as economic development and employment opportunities.
It is also the position of FNARF Board of Directors to have one representative (FNARF Funding Formula bases) from each of the Tribal/Brand Councils and Independent First Nations appointed to the Saskatchewan First Nations Resposible Gambling Technical Working Group (SFNRG-TWG) to provide recommendations which ensure effective Education, Prevention and Treatment in accordance with the FNARF mandate and mission.
Treatment Centres
Holistic Wellness Centre
Cottage 10 2300 9th Avenue West
Prince Albert, SK
TEL: 1-866-765-5305 or 306-765-5305
FAX: 306-763-5223
www.pagc.sk.ca or email: [email protected]
The MISSION is to provide support for problem gamblers, their families and community based education about problem and responsible gambling. The Holistic Wellness Centre focuses on Problem Gambling (inpatient/outpatient treatment) and is the only “stand alone” centre for the treatment of problem gamblers that is not based on ethnicity or residency. The Centre is located in Prince Albert, Saskatchewan.
White Raven Healing Centre
All Nations Healing Hospital
Fort Qu’Appelle, SK
TEL: 1-866-748-8922 or 306-322-2608
FAX: 306-332-2655
www.fhqtc.com
Our MISSION is to provide guiding principles that will encourage open communication with all individuals, families and communities. Our primary focus is to provide traditional and conventional therapeutic counseling designed to address the lagacy of intergenerational impacts of residential schools and unresolved trauma and family.
STC Health Centre
Gambling Addiction Services
1514 20th Street West Saskatoon, SK
S7M 0Z5
Phone: (306) 956.0340 Fax: (306) 956.0339
![]()
The Provincial Traffic Safety Fund Grant program enables projects to reduce traffic collisions, injuries and fatalities in communities across Saskatchewan.
Visit www.sgi.sk.ca/grantprograms for more information.









SGI Traffic Safety Partnership (TSP) Grant info sheet